Managed IT services for orthopedic offices means IT infrastructure designed around the specific demands of specialty care: PACS imaging networks that handle DICOM file transfers at volume, EHR integrations monitored in real time, HIPAA compliance maintained across every site and care partner, and cybersecurity coverage that includes imaging workstations that generic programs routinely miss. A general MSP can keep your email running. Orthopedic IT requires a different approach.
When your PACS goes down mid-clinic, you don’t call your general IT provider and wait. You lose imaging access, consultations stall, and your staff starts working around the system in ways that create compliance exposure. That’s the moment most orthopedic practices realize their IT infrastructure was built for a different kind of business.
This guide covers what managed IT services for orthopedic offices actually need to solve: imaging infrastructure, EHR integration, HIPAA compliance, multi-site connectivity, and cybersecurity risks that standard MSPs routinely miss.
Does Your Network Actually Support Your Imaging Volume?
Probably not, if it was not designed for it. A single MRI study runs 50MB to several hundred megabytes. DICOM files transfer differently from standard business data, and a network not sized for that traffic creates bottlenecks that interrupt clinical workflows. Most practices discover the gap when imaging delays become a daily complaint rather than an occasional one.
Multiply daily X-rays, CT scans, DEXA scans, and ultrasounds across your clinic volume, and your network moves serious data before lunch. Your Picture Archiving and Communication System (PACS) depends on that infrastructure performing without bottlenecks because a delay in pulling imaging before a consult is not a minor inconvenience. It interrupts clinical decision-making.
Most MSPs treat network infrastructure as a commodity. For orthopedic practices, it is not. Bandwidth sizing, latency management, and storage architecture for PACS require design around imaging volume. DICOM files, the standard format for medical imaging, transfer differently than typical business data, and a network not sized for that traffic will show it. If your IT partner has never provisioned for DICOM throughput, your infrastructure is probably undersized somewhere and you will find out at the worst possible time.
EHR integration carries the same logic. Your EHR communicates with your PACS via HL7 or FHIR interfaces, your billing platform, your scheduling system, and increasingly with external care partners. When those integrations break, the work does not disappear. It lands on your staff as manual re-entry, workaround communication, and delayed documentation. EHR integration managed services should monitor those integrations proactively, not respond to them reactively after your front desk notices something is wrong.
In a typical infrastructure engagement with an orthopedic practice, the first thing we find is an undocumented PACS server running on a network segment that was never formally sized for imaging volume. Nobody planned it that way. The system was added during a workflow transition, the original IT team moved on, and the bandwidth constraints became a slow background problem that everyone learned to work around. Fixing it is usually straightforward, but only after someone takes the time to map what is actually on the network.
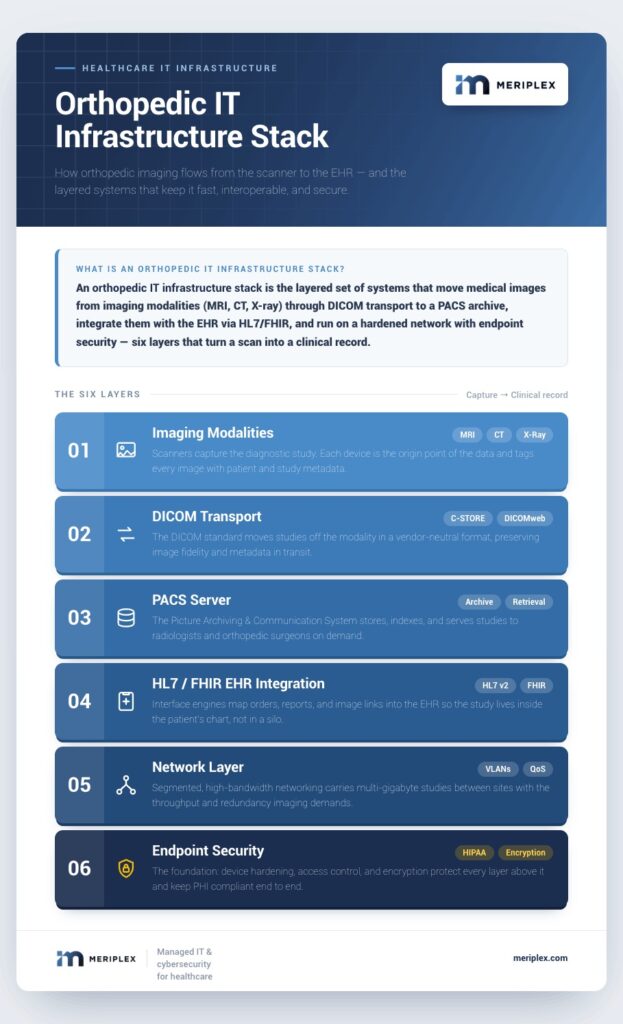
Orthopedic IT infrastructure is not a general business network with a healthcare label. It is a system built around DICOM throughput, HL7 integration points, and imaging workstations that standard security programs routinely overlook.
Your Imaging Infrastructure Has Specific Requirements. Let's See If Yours Are Met.
Where Does HIPAA Compliance Actually Break Down in Orthopedic Practices?
At the edges of your environment, not the center. Most practices have their EHR access controls in reasonable shape. The gaps appear in PACS servers running past vendor support windows, workers’ comp records transmitted without TLS encryption, and endpoints accessing patient records from outside the office without mobile device management enrollment. Each gap is individually manageable. Together, they represent the attack surface that healthcare breaches actually exploit.
Your PHI exposure surface in an orthopedic practice is wider than most compliance checklists account for. It includes:
- PACS imaging data stored on local servers or in cloud infrastructure
- Workers’ compensation and disability records
- Surgical documentation and implant data shared with device manufacturers
- Communication channels between your practice, referring physicians, and PT partners
- Every endpoint that touches patient records, including devices used outside the office
HIPAA compliant IT services for healthcare require audit-ready access controls, AES-256 encryption for data at rest and TLS 1.2 or higher for data in transit, annual NIST Cybersecurity Framework-aligned risk assessments, and a signed Business Associate Agreement (BAA) with every vendor who handles PHI, including your IT provider. If your current MSP has not executed a BAA with your practice, that gap exists today regardless of how well the helpdesk tickets get resolved.
The practices that end up in breach headlines are not usually the ones that ignored HIPAA outright. They are the ones that assumed a third-party vendor had adequate controls, or that allowed an unsegmented network to give ransomware lateral movement across clinical systems. According to the IBM Cost of a Data Breach Report 2025, healthcare has ranked as the most expensive industry for breach recovery for 14 consecutive years, now averaging $7.42 million per incident. Closing those gaps requires treating compliance as an ongoing operational discipline rather than an annual checkbox.
A signed BAA is table stakes. What actually protects an orthopedic practice is an IT partner who treats HIPAA as an ongoing infrastructure discipline: monitoring access logs, managing patch cycles on imaging systems, and governing third-party vendor sessions with the same rigor applied to internal endpoints.
Every Care Handoff Outside Your Clinic Walls Creates an IT Risk
Orthopedic care rarely stays in one building. A patient presents at your clinic, receives imaging at an affiliated facility, undergoes surgery at an ambulatory surgery center (ASC), then moves into physical therapy at a separate location. Each transition requires patient data to cross system boundaries, and each crossing is a point where security, compliance, and workflow can break down simultaneously.
ASC Connectivity
Your surgery center needs access to patient records, imaging, and implant documentation. When the ASC runs on a separate network with no secure integration to your clinic systems, staff compensate by faxing records, re-entering data manually, or using unsecured communication channels. Each workaround introduces PHI exposure and surgical preparation risk.
PT Clinic Data Sharing
Post-operative referrals to physical therapy require clinical information to transfer securely and accurately. In most practices today, this happens via fax or a patient portal that no one has formally reviewed for HIPAA compliance. A properly segmented network with encrypted SFTP or Direct Secure Messaging channels makes that transfer both faster and auditable.
Multi-Location Consistency
Growing orthopedic groups frequently add satellite offices and affiliated sites faster than their IT policies expand to cover them. One location without consistent endpoint management, access controls, and network monitoring is a breach vector for the entire organization, not just that site.
SD-WAN addresses much of this directly. It connects multiple sites, clinic, ASC, satellite offices, over a managed secure overlay network with consistent Quality of Service (QoS) policies, centralized firewall management, and real-time traffic visibility. For a multi-location orthopedic group, SD-WAN replaces the patchwork of site-by-site VPN configurations that most practices accumulate over time.
Operating Across Multiple Sites or Partnering with an ASC?
What Cybersecurity Risks Are Orthopedic Practices Most Likely to Miss?
Three surfaces that standard MSP security programs routinely underprotect: PACS and imaging workstations running past vendor patch support, EHR vendor remote access sessions with no formal governance, and remote endpoints enrolled in basic MDM but lacking endpoint detection and response (EDR) coverage and phishing-resistant MFA. Healthcare was the most targeted industry for ransomware in 2025, with 538 confirmed victims according to the Breachsense State of Ransomware 2025 Report.
According to the Breachsense State of Ransomware 2025 Report, healthcare was the most targeted industry for ransomware globally, with 538 confirmed victims, more than one attack per day. Orthopedic practices carry imaging records, surgical documentation, workers’ compensation files, and PHI volumes that exceed what most attackers expect from a specialty clinic. That combination of high-value data and lean internal IT staffing makes orthopedics a productive target.
For named breach cases and the specific threat patterns hitting orthopedic practices hardest, top 5 cyber threats targeting orthopedic practices covers that ground in depth.
Imaging Systems
HHS’s Health Sector Cybersecurity Coordination Center (HC3) has issued repeated warnings about unpatched PACS servers discoverable via open-source network scanning tools. PACS workstations frequently run specialized DICOM software on operating systems that cannot accept standard Windows Update patches without vendor validation, a process that can lag six to twelve months behind the patch release cycle. Security programs that treat these as standard endpoints miss how they are actually managed. Attackers do not miss this.
EHR Vendor Access
Your EHR vendor maintains persistent remote access to your environment for support and updates. Under HIPAA’s Technical Safeguard requirements (45 CFR Section 164.312), that access requires documented audit controls, unique user identification, and automatic logoff procedures. Most practices have the BAA in place but no formal governance over what the vendor’s session can reach or how long it stays open.
Remote Endpoints
Every device accessing patient data from outside the office requires MDM enrollment, EDR coverage, and phishing-resistant multi-factor authentication (MFA). Phishing-resistant means FIDO2 hardware keys or authenticator apps, not SMS one-time codes, which remain vulnerable to SIM-swapping and real-time phishing proxies. This is a baseline requirement, not an optional upgrade.
Managed Detection and Response (MDR) with a 24/7 Security Operations Center (SOC) provides the continuous monitoring layer that catches threats before they become incidents. For a practice running without a dedicated internal security team, MDR is the difference between isolating a compromised endpoint in minutes and discovering the breach days later when encrypted files and a ransom note are the first indication something went wrong. Meriplex deploys healthcare cybersecurity services that account for imaging workstations, EHR integrations, and remote access environments, not the generic endpoint stack built for a law firm or accounting practice.
For an orthopedic practice without a dedicated internal security team, MDR with 24/7 SOC coverage is the difference between isolating a compromised imaging workstation in minutes and discovering the breach when the ransom note appears.
What IT Support for Orthopedic Practices Looks Like When It Is Built for You
Here is the practical difference: a general MSP patches your workstations on a scheduled cycle and resolves helpdesk tickets. An MSP with healthcare expertise designs your network around PACS throughput requirements, monitors HL7 and FHIR integration points before they generate staff complaints, governs your ASC connectivity as part of your HIPAA compliance program, and covers your imaging workstations under the same EDR policy as your clinical endpoints.
That is not a higher tier of the same service. It is a structurally different service.
Meriplex works with healthcare and orthopedic practices to build IT environments matched to the actual complexity of specialty care: managed IT services for medical practices, cybersecurity, compliance management, cloud infrastructure, and the SD-WAN architecture that connects your clinic, your care partners, and your staff wherever they work.
If your current IT setup was designed for a general business and your practice has grown past it, the gap between what you have and what you need is not theoretical. It shows up in imaging delays, compliance exposure during audits, and the workarounds your staff have quietly built into their daily workflows to get through the day.