IT budgeting for healthcare organizations means allocating technology spend across three categories that behave differently than in any other industry: HIPAA compliance costs (broken into maintenance, readiness, and remediation), clinical uptime protection (calculated as revenue risk, not infrastructure overhead), and security spending benchmarked against healthcare-specific threat data. For mid-market organizations with 50 to 500 employees, a well-structured healthcare IT budget typically allocates 18 to 24% to security, separates compliance into three distinct line items, and treats a managed IT services model as a cost comparison against the fully loaded expense of in-house support.
Your organization had an IT incident last year that cost more than anyone budgeted for, and the fix came out of a line item that was supposed to cover something else.
If that sounds familiar, the problem probably isn’t that you spent too little on IT. It’s that the budget wasn’t built around the cost categories that actually drive risk in a clinical environment.
Most IT budget guides for healthcare don’t help with that. They recommend “investing in cybersecurity” and “modernizing your EHR” at a level of generality that applies equally to a dental office and a regional health system with 4,000 employees. Or they’re written for enterprise CIOs managing Epic implementations, organizations with entire IT departments to execute whatever the guide recommends.
If your organization sits somewhere between a single clinic and a 40-person IT department, you’ve probably closed a few of those articles without a single actionable number.
This one is built differently.
Want to Know Where Your Current IT Budget Has Gaps Before Your Next Board Conversation?
Healthcare IT Department Budget Benchmarks 2026
Healthcare IT budget planning for mid-market organizations requires allocating across categories that behave differently than in any other industry.
The table below consolidates the three cost categories and their benchmark ranges for organizations with 50 to 500 employees.
| Budget Category | What It Covers | Benchmark Range | Consequence of Underfunding |
|---|---|---|---|
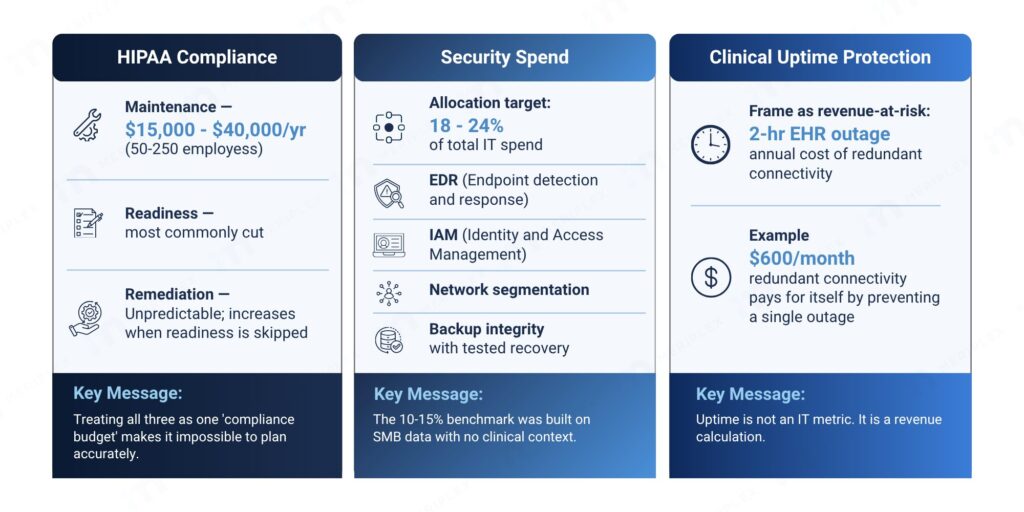
| HIPAA Compliance Maintenance | Continuous monitoring, BAA administration, access controls, audit log management | $15,000-$40,000/yr (50-250 employees) | OCR fines, documentation gaps, reactive remediation at emergency rates |
| HIPAA Compliance Readiness | Annual SRA, NIST SP 800-66r2 gap assessments, staff training, audit documentation | Most commonly cut line item; cost varies by org size | Missing documentation when a breach investigation begins |
| HIPAA Compliance Remediation | Gap closure after risk analysis findings; emergency fixes | Unpredictable; increases when readiness is underfunded | Compounds annually when compliance maintenance and readiness are skipped |
| Security Spend | EDR, IAM, network segmentation, backup integrity with tested recovery | 18-24% of total IT spend (healthcare-specific) | Increased breach exposure; cyber insurance premium increases |
| Managed IT Services Model | 24/7 monitoring, HIPAA expertise, defined SLAs vs. in-house IT generalist | $60,000-$90,000/yr (100-employee org) vs. $120,000-$160,000 in-house | Coverage gaps, reactive response, single point of knowledge failure |
| Clinical Uptime Protection | Redundant connectivity, DR solution sized to clinical revenue-at-risk | 2-hr EHR outage typically exceeds annual cost of redundant connectivity | Lost billable encounters, idle clinical staff, documentation liability |
The sections below cover each category in detail with the specific allocation logic and the questions to run before your next budget conversation.
The Budget Pattern That's Quietly Costing Healthcare Organizations
Compliance gets funded after a close call or a letter from the HHS Office for Civil Rights (OCR). Security spending gets sized by how nervous the leadership team feels after reading about the latest breach, not by any actual assessment of exposure. Infrastructure investment gets deferred until something breaks. And when a vendor proposes a managed services agreement, the CFO can’t evaluate it because no one has a baseline cost for the current model.
That’s reactive budgeting, and the cost compounds across every budget cycle. The dollars are there. They’re just arriving at the wrong problems at the wrong time.
According to the MGMA’s 2026 Medical Practice Excellence: Financial Operations report, medical group leaders are directing 30% of new budget dollars toward health IT initiatives, including AI tools, EHR upgrades, and cloud migrations. That’s a meaningful commitment. The problem isn’t willingness to spend. It’s that most organizations don’t have a framework that tells them how to allocate across the categories that actually matter in a clinical environment.
The categories that matter in a generic business are not the same ones that matter in yours.
What Should a Healthcare IT Budget Actually Include?
A healthcare IT budget should include at least four distinct cost categories that generic business frameworks miss: HIPAA compliance costs separated into maintenance, readiness, and remediation; clinical uptime protection sized by revenue-at-risk rather than infrastructure cost; security spending benchmarked against healthcare-specific threat data rather than cross-industry averages; and a managed IT cost comparison that accounts for the fully loaded expense of in-house support. Each category behaves differently in a clinical environment than it does in any other industry.
The most widely cited benchmark in IT budgeting content is the 10 to 15% security allocation, a number drawn from SMB data with no clinical context. It doesn’t account for HIPAA compliance costs as a distinct budget category. It doesn’t factor in what downtime costs per hour in a practice that bills by procedure. And it doesn’t distinguish between a manufacturing company that goes offline for two hours and a healthcare organization where that same outage delays patient care and triggers documentation liability.
For healthcare organizations, three cost categories behave differently than they do in any other industry, and most budget frameworks treat them as standard line items. They aren’t.
1. How Should Healthcare Organizations Budget for HIPAA Compliance?
Healthcare organizations should split HIPAA compliance spending into three separate budget lines: maintenance (ongoing controls and monitoring), readiness (annual risk analysis and audit preparation), and remediation (gap closure). Treating all three as a single “compliance budget” makes it impossible to plan accurately or catch underfunding before it becomes an OCR problem. For a 50 to 250 employee organization, compliance maintenance alone typically runs $15,000 to $40,000 annually when managed through a qualified IT partner.
Most organizations budget for “HIPAA compliance” as a single cost. In practice, it’s three separate categories with different drivers, different cadences, and different consequences if underfunded.
In a typical compliance engagement, the first thing we find is that a client has been funding remediation for years without realizing it. An access control gap surfaces during an internal review, someone calls in a favor to fix it quickly, and the cost lands in the general IT budget with no label. It happens three or four times a year. By the time we map it, they’ve spent more on reactive fixes than a structured readiness program would have cost, and they still don’t have the documentation to show an OCR auditor.
Healthcare organizations that collapse HIPAA compliance into a single budget line are almost always underfunding prevention and overpaying for remediation, often without realizing either is happening.
Compliance maintenance is the ongoing cost of staying compliant: continuous security monitoring, policy management, Business Associate Agreement (BAA) administration, role-based access controls, and audit log management. These map directly to the Administrative Safeguards under HIPAA Security Rule §164.308 and the Technical Safeguards under §164.312. This cost is largely fixed and predictable. For a 50 to 250 employee healthcare organization, expect this to run between $15,000 and $40,000 annually when managed through a qualified IT partner.
Compliance readiness covers the periodic work of proving you’re compliant: the annual HIPAA Security Rule §164.308(a)(1) risk analysis, gap assessments against NIST SP 800-66r2 (the HHS-endorsed implementation guide for the Security Rule), staff awareness training, and documentation reviews ahead of OCR audits or third-party assessments. Organizations subject to the HITECH Act, which strengthened HIPAA enforcement and introduced tiered civil penalties, face additional documentation obligations that fall squarely in this category. This is frequently the line item that gets cut when budgets tighten, and it tends to be what’s missing when a breach investigation begins.
The documentation OCR expects to find during an audit, including risk analyses, access control records, training logs, and BAA tracking, is covered in the HIPAA Compliance Checklist 2026 for Healthcare Providers.
Remediation is what you spend when a risk analysis reveals gaps that need to be closed. Organizations that skip readiness spending don’t avoid remediation costs. They just encounter them reactively, at emergency pricing, without the documentation trail that demonstrates good-faith compliance effort to regulators.
Treating all three as one “compliance budget” makes it impossible to plan accurately or defend the spending to a board. What the full healthcare cybersecurity regulatory stack actually requires in 2026 maps those obligations to the specific 45 CFR provisions OCR enforces, which is the right starting point for structuring each compliance budget line.
A formal Security Risk Analysis is required under HIPAA §164.308(a)(1) and falls under the compliance readiness category. How SRA and risk assessments differ explains what OCR specifically looks for in the deliverable and why the distinction matters for your compliance record.
2. How Much Does EHR Downtime Actually Cost a Healthcare Organization?
According to the Uptime Institute’s 2025 Annual Outage Analysis, more than half of significant outages cost organizations over $100,000 in direct impact. In a clinical environment where revenue depends on encounter documentation completed in real time, a two-hour EHR outage eliminates an entire morning of billable encounters, idles clinical staff, and generates hours of catch-up documentation work after systems come back online. That means a redundant connectivity solution costing $600 per month is not an IT expense. It is revenue protection, and for most mid-size practices, it pays for itself by preventing a single unplanned outage per year.
When an IT director says your organization needs redundant connectivity or a higher-tier disaster recovery solution, most CFOs pause at the price tag because no one has translated the investment into clinical financial terms. That translation is the missing step.
Research from the Uptime Institute’s 2025 Annual Outage Analysis found that more than half of significant outages cost organizations over $100,000 in direct impact. In a clinical environment where revenue depends on encounter documentation completed in real time, a two-hour EHR outage carries operational costs that typically exceed the annual price of the redundant connectivity solution that would have prevented it.
In healthcare, uptime is not an IT metric. It is a revenue calculation. Every hour of EHR downtime represents lost billable encounters, idle clinical staff, and documentation liability that no infrastructure investment could cost more to prevent.
That number changes the conversation. A redundant connectivity solution that costs $600 per month stops being an IT expense and starts being revenue protection. An infrastructure investment that prevents one outage per year likely pays for itself before Q2.
Aligning your IT budget with business goals means translating infrastructure costs into financial outcomes that a CFO or CEO can evaluate, not asking leadership to trust that uptime matters.
3. Security Benchmarks Need to Reflect Healthcare's Actual Risk Profile
The “10 to 15% of IT budget on security” guidance that circulates in general MSP content is a starting point for businesses where the primary risk is data loss or ransomware inconvenience. In healthcare, the risk profile is materially different.
Healthcare organizations were the most targeted sector for ransomware attacks in 2024, and according to the IBM Cost of a Data Breach Report 2023, the average cost of a healthcare data breach reached $10.93 million, more than twice the cross-industry average of $4.45 million. The cybersecurity threats hitting healthcare organizations hardest in 2026 covers what each attack type costs operationally and which HIPAA provisions it triggers, which is the right context for sizing your security allocation. Your security spend needs to be benchmarked against that exposure, not against a mid-size accounting firm’s threat landscape.
For mid-market healthcare organizations, roughly 3 to 30 locations with 50 to 500 employees, a practical security allocation looks closer to 18 to 24% of total IT spend, distributed across four categories: endpoint detection and response (EDR), identity and access management (IAM), network segmentation that isolates PHI-handling systems from general traffic (consistent with NIST SP 800-66r2 and the CIS Controls v8 framework), and backup integrity with documented and tested recovery procedures. Organizations adopting a Zero Trust architecture, which requires continuous verification of every user and device regardless of network location, should account for the additional IAM and micro-segmentation investment that model requires. Cutting any one of these categories to reduce cost typically increases exposure across the other three, particularly when IAM gaps allow lateral movement after an initial endpoint compromise.
Not Sure Whether Your Security Allocation Covers All Four Categories at the Right Threshold for a Clinical Environment?
The 10 to 15% security allocation benchmark was built on SMB data with no clinical context. Mid-market healthcare organizations facing a $10.93 million average breach cost need a security spend target that reflects their actual risk profile, not a generic industry average.
Cyber insurance underwriters are increasingly requiring documented evidence of EDR deployment, multi-factor authentication (MFA), and tested backup recovery before issuing or renewing policies in healthcare. If your security budget isn’t meeting those thresholds, the cost of non-compliance now shows up in your insurance premiums, not just your breach exposure.
The specific allocation within those categories should follow a formal risk assessment, not a percentage target. But if your current security spend is below 15% of total IT and you operate in a clinical environment, that gap is worth examining before something else prompts the conversation.
Whether a managed IT partner can actually deliver on that security allocation comes down to 10 specific capabilities. The ones most organizations forget to evaluate are covered in 10 must-have managed IT capabilities for healthcare.
What Does Managed IT Cost for a Healthcare Organization?
For a 100-employee healthcare organization, a fully loaded in-house IT model typically costs $120,000 to $160,000 annually once salary, benefits, training, tool licensing, and coverage gaps are included. A managed IT services model for the same organization typically runs $60,000 to $90,000 annually and includes 24/7 monitoring, HIPAA Security Rule expertise, and defined SLAs. The annual difference of $30,000 to $70,000 widens further when unplanned downtime and emergency response costs are factored into the in-house baseline.
“What does managed IT cost?” is a question most CFOs are thinking and few ask directly, because the answer requires an honest accounting of what the current model actually costs, including the line items that don’t show up on an IT invoice.
Here’s the comparison that changes the math. A fully loaded in-house IT model for a 100-employee healthcare organization, one IT generalist at market salary plus benefits, training, tool licensing, and the coverage gaps that open during PTO or turnover, typically runs $120,000 to $160,000 annually as a calculated estimate based on BLS median salary data for IT support specialists plus standard benefits loading. That model covers business hours, responds to tickets reactively, and gives you one person’s depth of knowledge across your entire environment.
A managed IT services model for the same organization typically runs $60,000 to $90,000 annually. For that, you get 24/7 monitoring, a team with working knowledge of the HIPAA Security Rule, HITECH breach notification requirements (72-hour reporting timelines under 45 CFR §164.410), and BAA obligations, plus defined SLAs for uptime and response time, and proactive maintenance that catches problems before they become outages. When evaluating managed IT providers, organizations operating in Microsoft 365 or Azure environments should confirm the provider carries relevant vendor certifications and can demonstrate SOC 2 Type II compliance, which signals that the provider’s own security controls have been independently audited.
That’s a $30,000 to $70,000 annual difference, before you account for the emergency hardware replacements, after-hours incident costs, and unplanned downtime that a reactive in-house model accumulates. A managed model converts those unpredictable spikes into a fixed monthly expense your finance team can plan around and your board can understand.
For healthcare organizations that have outgrown one IT generalist but aren’t ready to build a full internal team, this is the financial case for making a change: not a vague promise about “better support,” but a number you can put in a spreadsheet.
The specific questions to ask any provider before committing, covering HIPAA documentation depth, ransomware resilience, and subcontractor accountability, are what hospitals should ask HIPAA managed IT providers.
Four Questions to Run Before Your Next Budget Conversation
Before you engage any vendor or commit to any numbers, run these four questions with your leadership team. The answers will tell you more about where your budget needs work than any benchmark will.
- What would a two-hour EHR outage cost us this week? If no one can answer, your infrastructure investment decisions are being made without the financial context that justifies them.
- Can you separate your compliance maintenance costs from your remediation costs in last year’s budget? If not, you’re likely underfunding the former and absorbing the latter at emergency rates.
- When was your last third-party security risk assessment? If it’s been more than 18 months, your security spending is benchmarked against a risk profile that probably doesn’t reflect your environment anymore.
- What is your fully loaded cost for IT support today, including downtime, emergency fixes, and staff hours spent on IT issues? Most organizations haven’t added those line items to the salary figure. The calculation two sections above shows why that number matters, and why the managed IT comparison looks different when you use a real baseline instead of just the payroll line.
These questions won’t write your budget. But they’ll tell you which of the three cost categories above deserves the most attention, and give you the language to make that case to a board that’s used to hearing “we need more for IT” without a number attached.
If Your IT Budget Can't Answer These Questions, It's Not Done Yet
Most healthcare organizations heading into 2026 have an IT budget. Few have one that can answer what a two-hour outage costs, what percentage of security spend is allocated to identity management versus endpoint protection, or what the actual difference is between their current IT model and a managed alternative.
Those aren’t advanced questions. They’re the baseline for making defensible investment decisions, and they’re what separates a budget that holds up under board scrutiny from one that gets cut when something else needs funding.
The framework in this article won’t fit every organization identically. But the three cost categories, compliance split into maintenance, readiness, and remediation; uptime quantified in clinical revenue terms; security benchmarked against a healthcare-specific risk profile, give you a structure that reflects how healthcare IT costs actually behave. That’s a more useful starting point than any guide written for a generic 100-person business.
For organizations ready to evaluate what a managed IT services program would actually cost against their current model, the complete guide to managed IT services for healthcare is the right next step.